What is a deviated nasal septum?
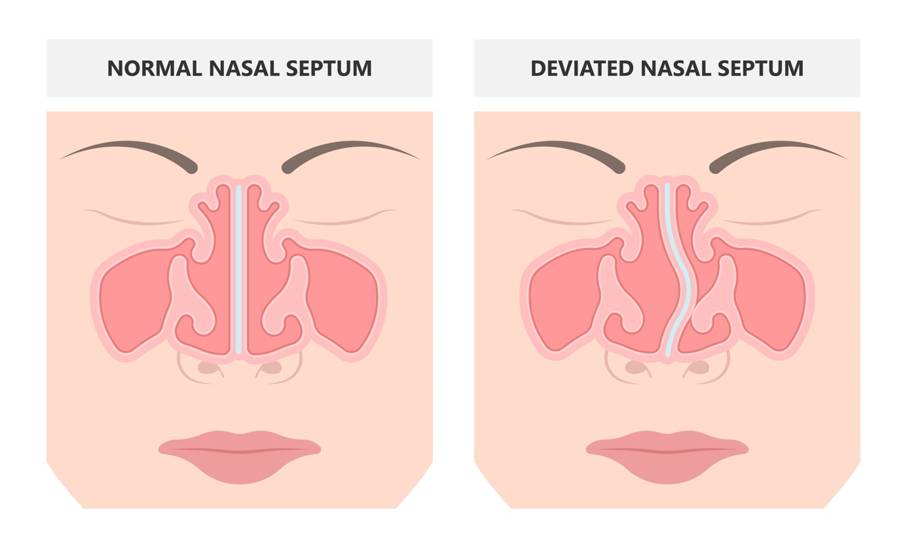
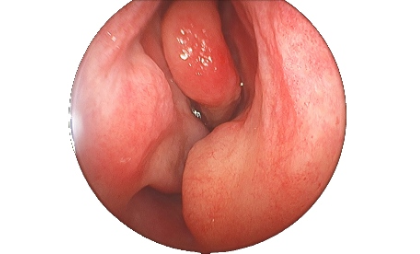
The nasal septum is the partition that separates the nose into two halves. It is made up of cartilage and bone. As many as 15% of the population will have a deviation of the nasal septum causing restriction in breathing through one or both sides of the nose. The nasal septum is a 3-dimensional structure and thus deviations can occur in any direction
How did I get a deviated nasal septum?
Nasal septal deviations can occur as a consequence of nasal trauma but sometimes there is no obvious cause. Some people believe that trauma during childbirth can predispose to a deviation later on in life.
What are nasal turbinates?
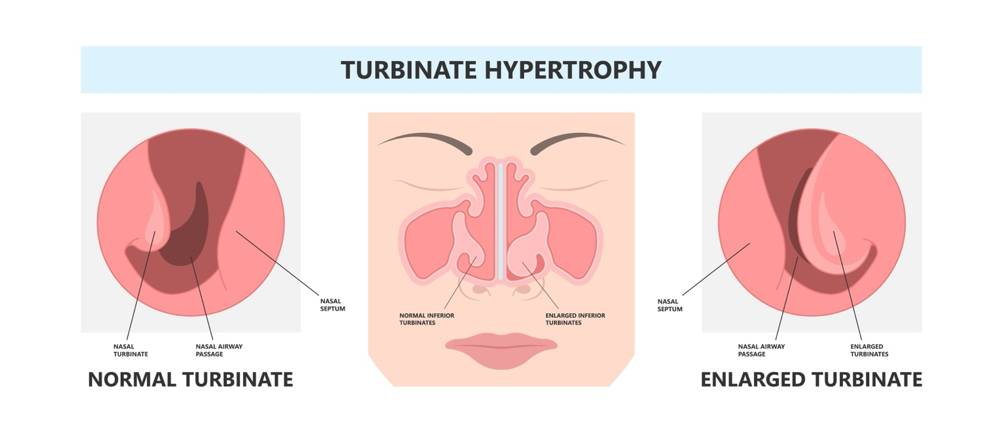
We have paired fleshy structures running through the nose. The largest of these are known as the inferior turbinates. The turbinates are bony structures covered with mucous membranes and can become enlarged because of inflammation, allergy or sometimes after using nasal decongestants for a prolonged period. Enlarged turbinates cause nasal obstruction and congestion. Occasionally, individuals are aware of alternating nasal obstruction.
How is a Nasal Septoplasty performed?
The procedure is performed under general anaesthesia and normally takes between 30 and 45 minutes in total. Medicines that constrict blood vessels are used in the nose to reduce any bleeding during the procedure. A single incision inside the nose is used to access the cartilage and bone that make up the septum. The excess / deviated tissue is removed taking care not to disrupt the important structural supports of the nose, allowing the septum to sit within the midline. A dissolvable running stitch is used to hold everything in place and close the incision
What are the risks of Septoplasty?
Bleeding. This is commonly encountered and occasionally requires the placement of packs to reduce bleeding in the immediate postoperative period. Packs exert pressure on bleeding areas and are usually removed 3-4 hours after surgery.
Infection. This occurs in less than 1% of cases and feels like a bad cold. Very rarely, infection can be serious so it is important to seek advice if pain and discomfort increase as you are recovering.
Change in shape of nose. This occurs in less than 1% of cases and is more common if the septal deviation is very severe. The commonest problem is a dip in the bridge of the nose and this risk is minimised by the surgeon taking care not to alter the structural supports of the nose.
Revision surgery. Approximately 1 to 5% of individuals will experience some residual or recurrent deviation and may need to undergo further surgery
Septal Perforation. Rarely a hole can be created within the nose linking one side to the other. The overall risk of this occurring is about 1%. A small proportion of people with this complication could experience bleeding, crusting or a whistling sound when breathing through the nose. It may be corrected by further surgery.
If I need turbinate surgery, how is this performed?
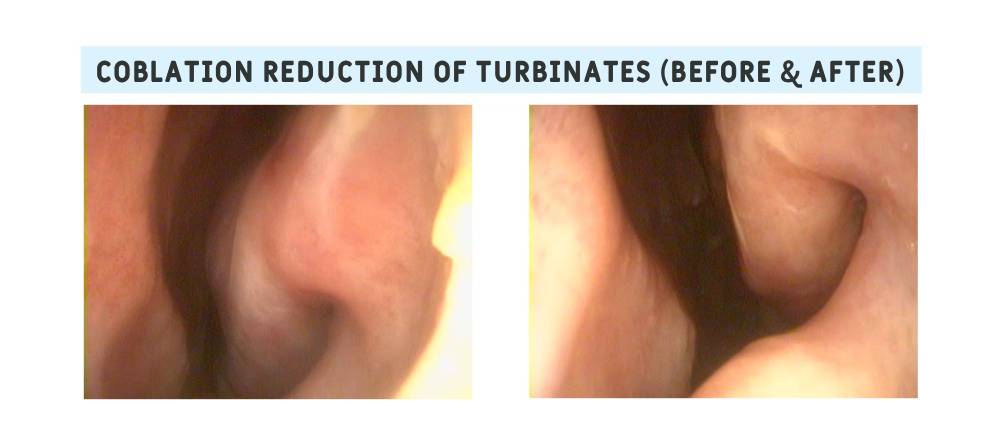
There are many different techniques to reduce the size of the inferior turbinates. Our preferred technique is to use Coblation ® of the turbinates. Coblation ® uses a special plasma derived from saline (salt water) to break down tissue in a very precise manner. The changes to tissue take place at around 40oC, resulting in very little heat transfer to the surrounding tissue, thereby reducing complications and pain.
What are the risks of Coblation turbinate reduction?
The risks of this method are similar to the risks of bleeding encountered during sepal surgery and are managed in the same way
What to expect after surgery?
Nasal obstruction is normal for up to two weeks following the operation. Crusting and bleeding are often experienced during this time. Numbness at the tip of the nose is very common and almost always resolves over time.
What treatments should I use after surgery?

Nasal decongestants such as Otrivine (prescribed or obtainable over the counter at most pharmacies) should be used for 5 days only. Treatment for any longer than this period can be detrimental to the nose. A salt water nasal rinse such as NEILMED SINUSRINSE® or STERIMAR® can be very effective in speeding up the recovery following surgery and helps reduce post operative complications. It should be used twice daily for at least 2 weeks but can be used for longer if needed.
Paracetamol and Ibuprofen should be taken regularly for the first one week and then can be taken as required until all discomfort has settled.
Other useful post-operative advice
For the first few days, try not to blow your nose. If you need to sneeze, try to do so with your mouth open. Try not to over exert
yourself for two weeks as this could lead to bleeding. Driving is safe after 24 hours. A follow appointment is usually booked for two weeks after surgery.